
The medical charts on Miguel Ondetti’s desk told a story of quiet desperation. In the early 1970s, treating high blood pressure felt less like healing and more like trading one disaster for another. Patients survived the immediate threat of stroke, only to collapse into crushing depression or suffer sudden, violent electrolyte crashes that left them weak and confused. Ondetti and his colleague David Cushman watched these files pile up at Squibb, feeling the weight of every name. They weren't just looking for a better molecule; they were looking for a way to stop hurting the people they were supposed to help.
They abandoned the standard chemical playbooks and looked to the jungle. The Brazilian pit viper, Bothrops jararaca, possessed a terrifying efficiency: its venom dropped prey's blood pressure instantly, causing shock. It was a survival mechanism for the snake, but for Ondetti and Cushman, it was a blueprint. By 1971, they had isolated the active peptides from the venom. These natural compounds blocked the body’s pressure-raising pathway with elegant precision. But there was a catch. The peptides dissolved in the bloodstream within minutes. The snake’s gift was brilliant, yet utterly useless for a patient who needed protection twenty-four hours a day.
The real enemy was not the venom, but the body’s own engine: the Angiotensin-Converting Enzyme, or ACE. Imagine ACE as a relentless factory worker, stamping a "tighten" order on artery walls every few minutes. To stop this worker without shutting down the entire factory, they needed to understand his grip. Ondetti and Cushman mapped the enzyme’s active site, searching for a weakness. They found it in the center: a single zinc atom, exposed and vulnerable. If they could lock onto that zinc, they could freeze the worker’s hand mid-stamp.
Designing the key required a shift from observation to engineering. They crafted a synthetic molecule featuring a sulfur-hydrogen anchor. This specific chemical group was designed to clamp onto the zinc ion like a rust-proof padlock. The goal was a targeted blockade: stop the pressure-raising cascade without harming the kidneys or clouding the brain. It was a delicate balance. Too weak, and the blood pressure would spike again. Too broad, and they would repeat the side effects of the old drugs.
The lab bench became a place of endless frustration and minor adjustments. They tweaked the carbon backbone, testing each draft in petri dishes. They refined the angles of the molecule, trying to make it survive the harsh acidity of the human stomach while holding firm in the blood. For months, the results were ambiguous. Then, the data shifted. The synthetic key finally fit. It didn't just bind; it held. The enzyme was neutralized, not destroyed, allowing the body’s other systems to function normally.
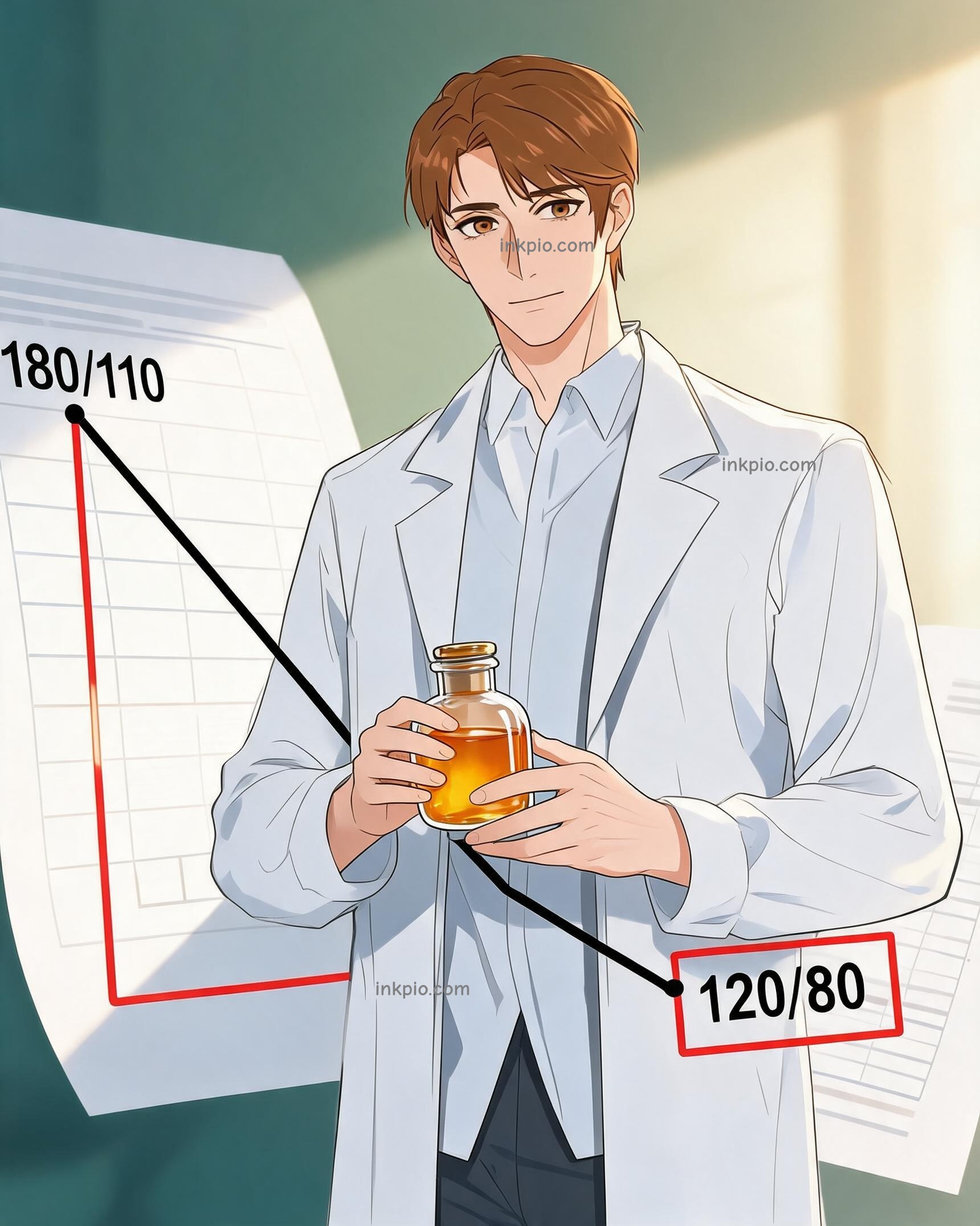
Clinical charts began to paint a different picture. Patients took the new tablet, and instead of the usual crash, their readings slid safely from crisis levels to a steady baseline. There were no mood swings. No dangerous mineral losses. Just a quiet, precise chemical switch that worked as planned. For the first time, the treatment felt like a partnership with the body rather than an assault on it.
In 1981, Captopril cleared FDA hurdles, becoming the first orally active ACE inhibitor. Ondetti and Cushman stood by as the first production batch rolled out. The atmosphere in the lab was not one of raucous celebration, but of exhausted relief. They quietly closed their notebooks. The jungle’s brutal survival trick had been tamed, refined, and packaged. It now sat in medicine cabinets, waiting. Somewhere, a patient would swallow a small white pill, unaware of the zinc atom locked inside, unaware of the years of failure that preceded it. They would simply feel their heart beat a little easier.